Estimated U.S. prevalence of these diseases is 600 to 2,500 individuals.
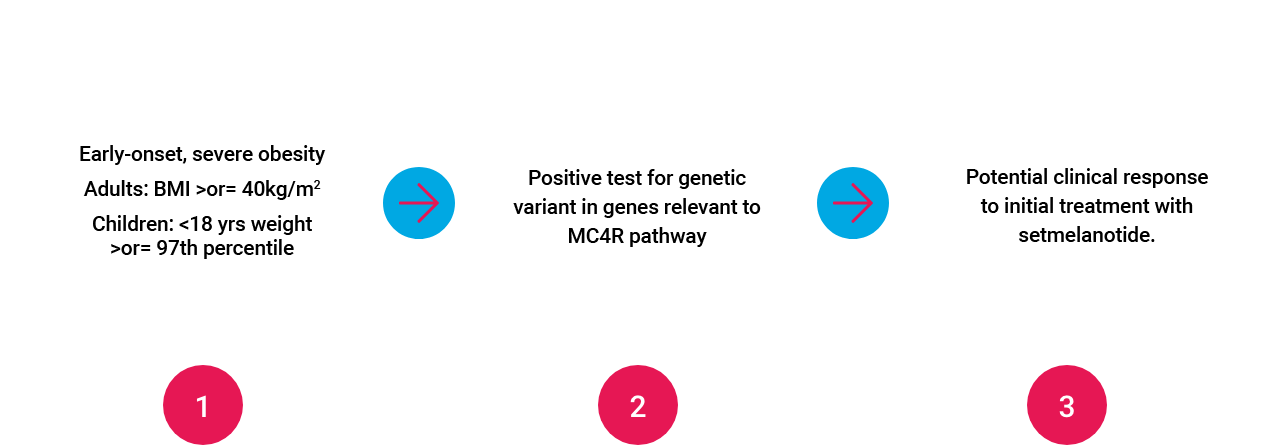
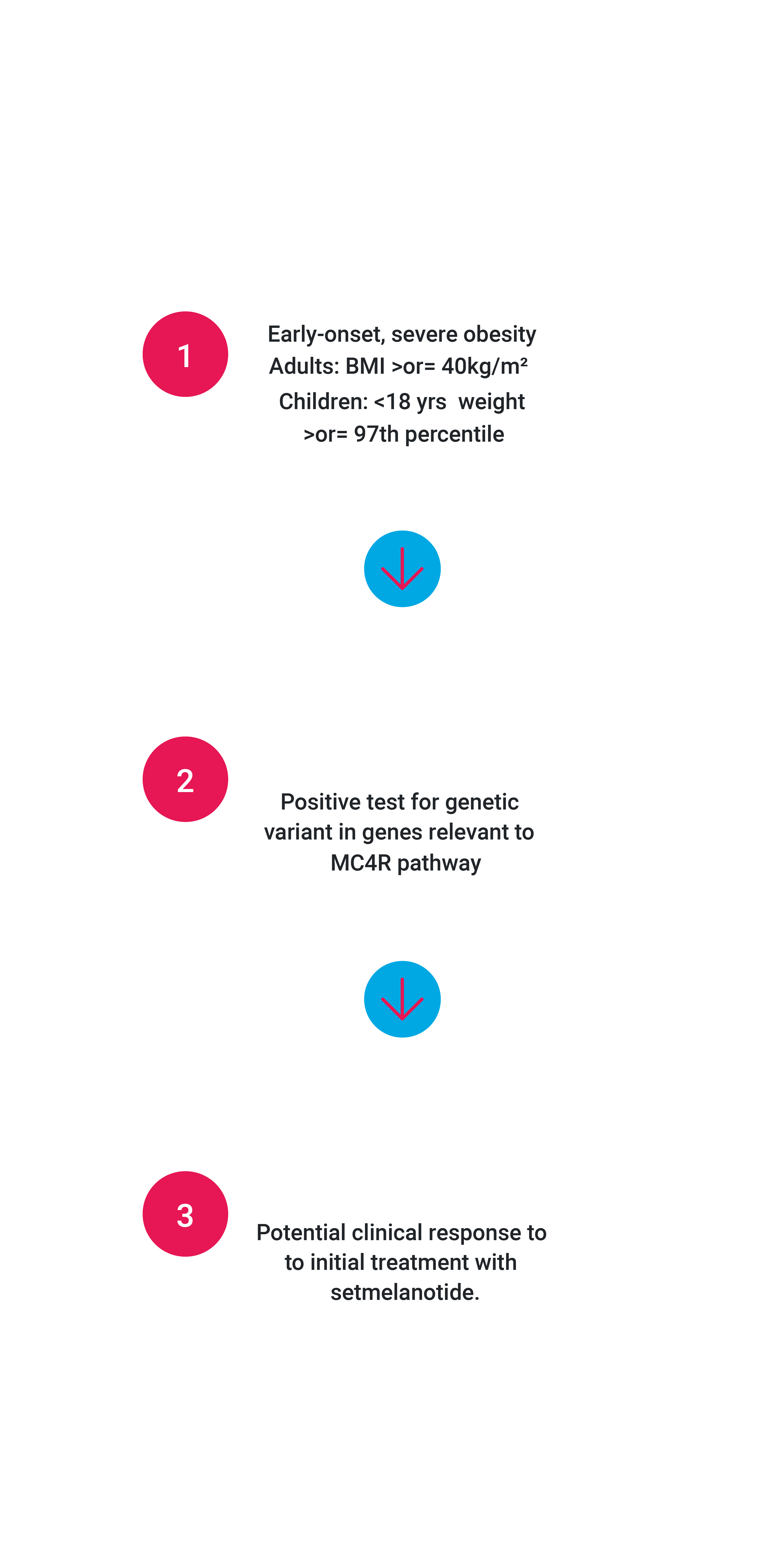
We have completed two Phase 3 trials evaluating setmelanotide in these diseases. Obesity due to POMC or LEPR deficiency are ultra-rare diseases caused by variants in POMC, PCSK1 or LEPR genes that impair the MC4 receptor pathway, which is a pathway in the hypothalamus that is responsible for regulating hunger, energy expenditure and consequently body weight. People living with obesity due to POMC or LEPR deficiency struggle with extreme, insatiable hunger beginning at a young age, resulting in early-onset, severe obesity. For more information, visit IMCIVREE.com